
Fall Prevention
- Kristi Riker
- 2 days ago
- 5 min read

Fall Risk with PD
Higher fall risk is a daunting but sometimes inevitable part of life when living with Parkinson’s disease. A comprehensive review found that “45–68% of people with Parkinson's experience at least one fall each year, roughly three times the rate of healthy older adults” (Murueta-Goyena, 0224). Around half of those falls lead to secondary injuries including fractures and head injuries. Those who experienced recurrent falls reported a wide range about 5-60 falls per person per year. This shows just how severe fall risk can become with advanced PD.
Predictors of falling:
Previous fall history
This is the strongest predictor because it indicates that mobility, balance, and/or cognitive factors are already present (Bradley, 2025)
Gait abnormalities
Short shuffling steps, reduced arm swing, gait variability, and difficulty turning make tripping and loss of balance more likely.
Postural instability
Impaired postural reflexes make it harder to recover from a loss of balance.
Freezing of gait
Sudden inability to move the feet can cause forward falls, especially during turning, doorway crossing, or multitasking.
Greater disease duration and severity
Motor and non-motor symptoms accumulate over time, increasing instability and mobility limitations.
Cognitive impairment
Reduced executive function and attention make it harder to safely navigate obstacles and multitask.
Autonomic dysfunction (blood pressure drops suddenly)
Orthostatic hypotension can cause dizziness, lightheadedness, or fainting when standing, leading to falls.
Decreased reaction time
If a Fall Occurs:
If a fall occurs, first stay calm, check for injuries, and avoid trying to get up quickly if you feel pain, dizziness, or cannot move safely. If you are able, roll to your side, move to your hands and knees, use a stable chair or surface for support, and slowly return to standing or call for assistance if needed.

Potential Consequences of Falling
Approximately half of falls in people with Parkinson's result in an injury. Recurrent falls are common and can have significant physical, psychological, and functional consequences.
Potential Physical Consequences:
Fractures, especially hip, wrist, and vertebral fractures
Head injuries, including concussion
Soft tissue injuries (bruises, sprains, cuts)
Increased pain and reduced mobility
Longer recovery times compared with older adults without Parkinson's
Increased risk of complications after injury, such as deconditioning and loss of muscle strength
Physical inactivity following a fall - muscle weakness and worsening balance from reduced activity
Increased future fall risk
Potential Psychological Consequences:
Fear of falling (FOF), which is very common after a fall
Loss of confidence in walking and performing daily activities
Anxiety about leaving the home
Depression and reduced self-esteem
Hospital and ER visits - stress of healthcare costs
Reduced desire to participate in exercise or social activities
Potential Daily Function Consequences:
Reduced independence in activities of daily living
Greater reliance on caregivers
Difficulty performing tasks such as bathing, dressing, shopping, and community mobility
Reduced participation in work, hobbies, and recreation
Increased use of assistive devices
Potential need for assisted living or long-term care placement
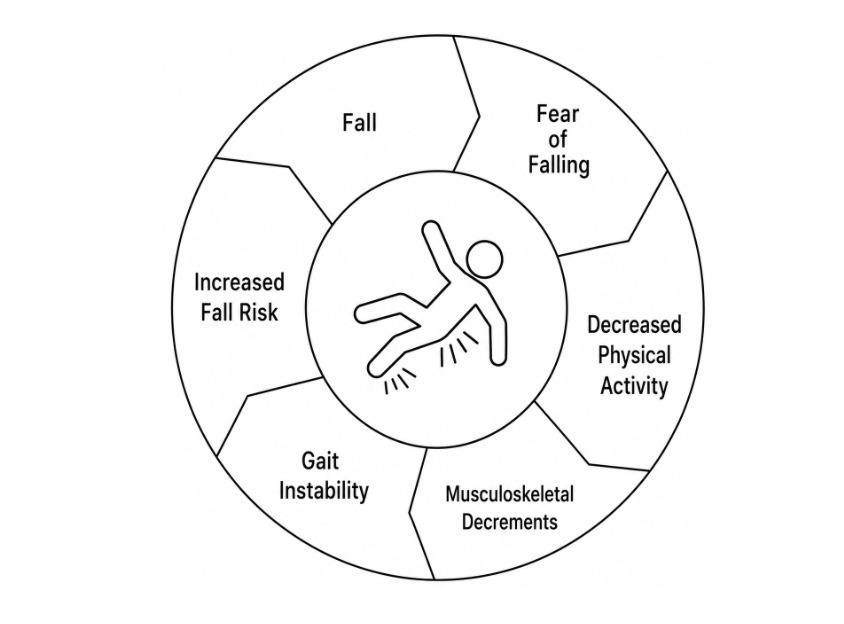
The Fall Cycle
A single fall can initiate a cycle of fear, inactivity, physical decline, and increasing dependence, ultimately compromising an individual's ability to live independently.
How to Prevent Falls
How do we actually prevent falls from happening? First, it’s crucial to be aware of your own fall risk. Fall risk is typically categorized as low, moderate, or high. A healthcare provider - most often a physical therapist can assess an individual’s fall risk using a combination of questionnaires and standardized assessments. They should observe gait, balance, freezing, cognition, fall history, medications, fear of falling, home environment, and conditions such as orthostatic hypotension. This multifactorial approach provides a more complete picture of an individual's fall risk than any single test and helps clinicians tailor interventions to the person's specific circumstances.
Fall Risk Assessments:
While most research-backed fall-risk assessments require observation by a healthcare provider, there are free online fall risk screenings. These can help individuals with PD screen their risk to discuss concerns with their provider.
Free online fall screenings:
Evidence-Based Interventions to Decrease Fall Risk
Evidence-based interventions to reduce fall risk in people with PD focus on improving mobility, balance, and overall physical function while addressing individual risk factors. Research consistently shows that no single intervention is sufficient; instead, multifactorial, individualized intervention is the best approach to preventing falls.
A fall prevention program should include a combination of interventions such as these:
Physical and occupational therapy
PT and OT teach exercises to improve gait, posture, strength, flexibility, and balance. They also teach strategies for safe movement, turning, transfers, and fall recovery.
Bridges for Parkinson’s Fitness Program
All classes are largely focused on fall prevention and target skills such as turning corners, dual tasking, and overall strengthening.
Cueing strategies
External cues such as rhythmic sounds, metronomes, counting, laser lines, or floor markings help overcome freezing of gait and improve walking rhythm and step length.
Exercise and balance training
Enhances muscle strength, postural control, coordination, and reaction time, reducing instability and improving the ability to recover from balance disturbances.
Home modifications
Reduces environmental hazards by removing clutter, securing rugs, improving lighting, installing grab bars, and creating clear walking paths to decrease trip and slip risks.
Wearable monitoring technology
Sensors and smart devices can detect gait changes, monitor balance, identify high-risk periods, provide real-time feedback, and alert caregivers after falls, enabling earlier intervention.
Fall prevention exercise
For fall prevention in Parkinson's disease, the strongest evidence supports a multicomponent program that combines aerobic exercise, strength training, balance training, and gait-specific practice rather than relying on a single exercise type. Bridges for Parkinson’s Fitness Program includes all of the exercises in the routine below.
Sample Parkinson's Fall-Prevention Exercise Routine
Exercise | How to | Purpose | Amount | Frequency |
Large amplitude walking | Walking with long steps and arm swing | Improves gait, speed, and stride length | 5-7 days/week | 20-30 min |
Strength training | Sit-to-stands from chair; squats to chair; calf raises; resistance band rows; hip abduction exercises | Improves lower body strength for balance recovery | 3 sets of 10 each; 2-3 days/week | 20-30 min |
Balance training | Tandem stance (heel to toe); single leg stand; reaching tasks in standing; pivot practice | Improves postural control and reduces fall risk | daily | 10 min |
Stretching | Trunk rotations; hamstring stretches, calf stretches; chest opening, neck mobility | Reduces rigidity and improved movement efficiency | daily | 10-15 min |
High-value activities | Boxing; Tai CHi; Yoga; Dance; Cycling; Virtual Reality | Improve balance, coordination, mobility and confidence | 2-3x/week | 30-60 min |
(From current Parkinson's rehab recommendations; should be individualized by a healthcare provider.)
Future Directions in Fall Prevention for Parkinson’s Disease
Fall prevention for individuals with PD is moving toward more personalized, proactive, and technology-supported approaches. There have been advances in the use of wearable sensors, artificial intelligence, and remote monitoring. These technologies may aid in earlier identification of changes in gait, balance, and mobility before falls occur. Future rehabilitation strategies are expected to focus on individualized exercise programs, including advanced balance training, dual-task activities, reactive postural control, and virtual reality–based interventions to improve real-world mobility. Smart home systems are used more often than ever for fall detection and prevention. These include fall motion sensors and voice activated assistants which alert caregivers in the case of a fall. As these methods develop, one finding remains essential for fall prevention - a multidisciplinary approach combining neurologic care, therapy, exercise, and technology is the best way to maintain safety and independence for people with Parkinson's disease.
Resources:
Bradley, M., O’Loughlin, S., Donlon, E., Gallagher, A., O’Keeffe, C., Inocentes, J., Ruggieri, F., Reilly, R. B., Walsh, R., Lynch, T., Di Luca, D. G., & Fearon, C. (2025). Determining Falls Risk in People with Parkinson’s Disease Using Wearable Sensors: A Systematic Review. Sensors, 25(13), 4071. https://doi.org/10.3390/s25134071
Fan, X., Yuan, Y., Bai, Y. et al. Optimal dose and type of exercise improve the overall balance in adults with Parkinson’s disease: a systematic review and Bayesian network meta-analysis. Neurol Sci 46, 4169–4180 (2025). https://doi.org/10.1007/s10072-025-08244-1
Murueta-Goyena, A., Muiño, O. & Gómez-Esteban, J.C. Prognostic factors for falls in Parkinson’s disease: a systematic review. Acta Neurol Belg 124, 395–406 (2024). https://doi.org/10.1007/s13760-023-02428-2
Stewart A Factor, David Weinshenker, and J Lucas McKay. A possible pathway to freezing of gait in Parkinson's disease, Volume 15, Issue 2 (2025), https://doi.org/10.1177/1877718X241308487

Comments